

Misinformation Monitor (Part 2)
The MHRA knew early in 2021 that there were high levels of ADRs. ADRs were particularly high in the vulnerable group of pregnant women, who the MHRA are specifically charged to protect.

INTERIM REPORT (July 2021)
In the MHRA's reply to my FOI in July 2023, I was sent an Interim Report on the YCVM. This was a presentation given to the Pharmacovigilance Expert Advisory Group (PEAG) of the CHM, at a meeting in July 2021. The PEAG purpose is to assesses risks of medication to the public but there was no reaction to the high level of adverse drug reactions (ADRs) seen in pregnant women recorded.
This was the only Monitor report available until the Pre-Print in November 2024. The Interim Report data was known by the MHRA in July 2021, nearly 4 years ago, and contradicts the SmPC which MHRA updated on 21.3.24: “There were no vaccine-related effects on female fertility, pregnancy, or embryo-foetal or offspring development.”
Why does the MHRA not acknowledge the high level of ADRs in this Monitored pregnancy group (a vulnerable, special group that they are charged with protecting), as a strong signal that needs investigating?
This Interim Report has been analysed by Prof Norman Fenton, a mathematician who is a world leading expert on risk assessment and statistics with a focus on Bayesian probability. His report shows that in the MHRA data supplied, including 1366 pregnant women in the YCVM, with 41% (565) reporting at least one ADR. "Of those who received the Astra-Zeneca vaccine a whopping 66% (124 out of 203) reported at least one ADR; 38% of the Pfizer recipients and 61% of the Moderna recipients reported at least one ADR. They are therefore hiding pregnant women's data, that is indicating potential harm, which is scandalous."
Why is it acceptable for pregnancy data to not be disclosed, analysed, and acted on until after publication (nearly 4 years after the rollout)?
MHRA Guidance on Pregnancy 6.2.25. States:
There is no known risk with giving inactivated virus or bacterial vaccines or toxoids during pregnancy or whilst breast-feeding.
The JCVI has advised that pregnant women should be offered COVID-19 vaccines at the same time as people of the same age or risk group.
The MHRA has raised no specific concerns for safety in pregnancy.
Nothing to see here. No evidence given to back up what is stated. The MHRA have not changed their assessment of the Benefit/Risk Ratio despite their own evidence of unprecedented number of serious ADRs in the Monitor, and they are still recommending in pregnancy. Prof Fenton, ‘The Statistical Illusion of Better Pregnancy Outcomes for Vaccinated Women’ (2022)
Why are MHRA not using the evidence of the Monitor? Where is their evidence allowing MHRA to make these statements?
Information available at the time of the Interim Report:
The harm is shown with the 41% of the pregnant cohort showing at least 1 ADR in the Interim Report.
The harm is shown in the Yellow Card Reports by July 2021 with 965,437 ADRs (283,434 reports) and 1328 fatalities.
It is important to note the Adverse Events in the Pfizer (5.3.6) document, the 90-day post-marketing period starting on 1 December 2020, show 1,223 deaths.
ADRs of the PRE-PRINT
13.7% experienced a medically serious ADR because of these "safe and effective" products.
53% of participants reported at least one ADR;
22% of ADRs affected everyday activities (0.5%=hospitalisation; 0.3%=disabling; 0.1%=life-threatening).
ADRs are listed on 221 pages with no discussion or analysis.
Pregnancy:
The maternal/perinatal outcomes in pregnancy data are essential; but not presented at all.
41.2% of pregnant women reported at least 1ADR but with no further discussion on seriousness.
8 cases of congenital anomaly are listed but there is no detail to evaluate these cases.
Pregnancy ADRs are listed on 73 pages with no discussion or analysis.
MHRA's role is PHARMACOVIGILANCE (drug safety)
MHRA states: "We keep watch over medicines and devices and take necessary action to protect the public promptly if there is a problem". MHRA has a duty of care to act in the Public Interest:
to act on any data of harm
to make information available to the public promptly
to reduce the possibility of serious injury.
MHRA always remind us that the Monitor was only one of the four main strands of MHRA's proactive vigilance to assess new safety signals:
Enhanced Passive Surveillance - “observed vs expected” analysis = Yellow Card
Rapid Cycle Analysis & Ecological Analysis
Targeted Active Monitoring = YCVM
Formal Epidemiological Studies
Yellow Card Scheme, now 60 years old, run by the MHRA, to share "suspected" adverse drug reactions (ADRs) to medications including vaccines and devices and others. The MHRA published regularly the Covid-19 vaccine Yellow Card data. They state the purpose of the scheme is to provide an early warning on safety of a product which may require further investigation. It is described as enhanced passive surveillance but only 1-10% of ADRs get voluntarily reported by the public and health care professionals.
But what happens to this reported data? In an answer to the Internal Review of FOI 22/562, “The MHRA does not hold a process for investigation of individual Yellow Card reports.” Those who submit a Yellow Card report rarely hear anything further - they have effectively disappeared in the system. Dame Cumberlege (21mins) said the public believe reports end up in the bin!
The analysis is based on ‘observed vs expected’ data. The Yellow Card scheme underpins medicine and vaccine safety monitoring in the UK. In Pursuing a death report, this reporter states, "I can only conclude that the MHRA is hopelessly inept or wilfully blind. I suspect both. The Yellow Card system is supposed to “rigorously” and “continuously” “monitor information on suspected safety concerns”
The MHRA make 4 telling statements, seen by everyone completing a Yellow Card report (or the YCVMonitor):
The existence of an adverse reaction report does not necessarily mean that the vaccine has caused the reaction.
Sometimes, reactions can be part of the condition being treated rather than being caused by the vaccine.
Many factors have to be considered when assessing whether a vaccine has caused a reported adverse reaction.
It is important to note that most people receive vaccinations without having any serious side effects.
The MHRA assumption is that the cause cannot be the Covid-19 vaccines.
- but they never investigate the correlations and indications of causality. Causality was shown by Dr Peter McCullough and Dr Jessica Rose based on VAERs data used in the Bradford-Hill criteria accepted by WHO. If the tenants of causality can be shown here and here, then why are all Regulators including the MHRA, not even looking and therefore turning a blind eye?
Dr Tess Lawrie, in a letter to Dr June Raine at the time of the Interim Report, stated: "The MHRA now has more than enough evidence on the Yellow Card system to declare the COVID–19 vaccines unsafe for use in humans". Yellow Card reports (26th May 2021), with pregnant women comprising a small proportion of the UK vaccinated population, show a high number of Pregnancy ADRs (307 ADRs), including one maternal death, 12 stillbirths and 150 spontaneous abortion".
Dr Tess Lawrie wrote to the MHRA again in August 2021, "We ask the MHRA to take action as follows, in line with its statutory obligation to minimise risk to individuals~
Suspend the COVID-19 vaccines immediately in all children
Suspend the use of COVID-19 vaccines in all adults
Suspend enrolment in trials in UK of COVID-19 vaccines
Postpone any EUA assessment of booster vaccinations
Conduct a comprehensive overhaul of the UK’s Yellow Card system
What has happened to pharmacovigilance when the MHRA are stating that people should still be vaccinated even though they have their own Monitor data that indicates 1 in 7 develop severe ADR?
THE V-SAFE MONITOR
The same monitoring system was used in the US, (V-Safe), but with 10million participants. Similarly to the MHRA, the CDC would not release the V-Safe data, but Informed Consent Action Network (ICAN) sued, and they were court ordered to release the data in September 2022. This was a release of more than 151million health surveys about experiences following Covid-19 vaccination.
The V-Safe data shows that 25% were incapacitated the day after vaccination. Overall, 7.7% (770,000) of the 10m participants had a serious health event reporting that they needed medical care after getting the vaccine on average 2-3 times each. Over 70% of them required medical attention, emergency room intervention and/or hospitalisation.
Similarly, but worse, 97% of the 35,691 pregnant women in the V-safe database and their babies who were injected with the experimental gene therapy drug, had no outcomes recorded.
Again, this real time data is throwing up large numbers of ADRs, like the Interim Report and the YCVM data. This was not just recorded in the UK as it is a global problem. As with the MHRA, the CDC ignored these reports from its own V-safe program, but it has also ignored studies from healthcare specialists within the United States supporting these same harms. For example, one study found significant harms to pregnant women and infants following COVID-19 vaccination during pregnancy. The release of the data in the fourth V-Safe production reveals a disturbing trend in miscarriages and menstrual disturbances following covid-19 vaccination.
The publication of data in peer reviewed journals has also been a route taken by the CDC. (Shimabukuro et al). Preliminary finding of the mRNA COVID-19 Vaccine Safety in Pregnant Persons. NEJM. Apr 2021. Recently, Senator Ron Johnson has indicated that Dr Shimabukuro (CDC Vaccine Safety Director), has been implicated in the concealment of an 82% miscarriage rate among Covid-19 vaccinated women in this study - the reports “remain lost”. According to ICAN all studies published on V-Safe only cover one week after vaccination.
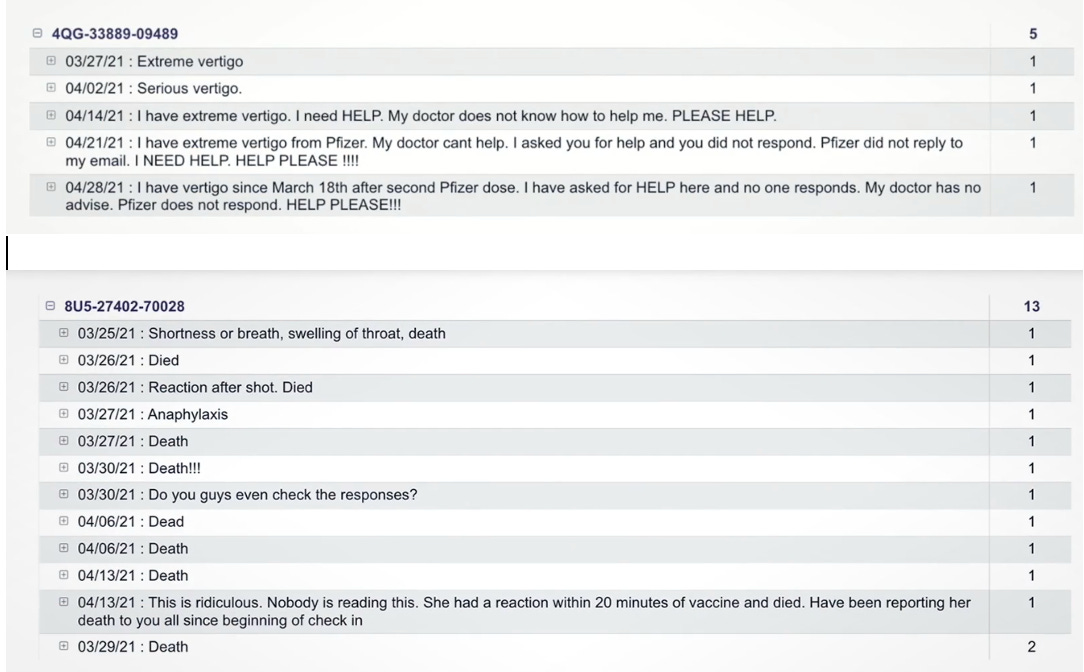
MHRA have not released or discussed the critical “free text” entries collected. The CDC have again been court ordered by a federal judge, to release the 7.8m free text entries from V-Safe, which again had never been disclosed.
V-Safe free text reports were released via the Highwire and ICAN who obtained the data. Cries for help from a Vertigo Report and a Death Report:
SAFE & EFFECTIVE
The MHRA continues using the word "safe". Dr Alison Cave, Chief Safety Officer MHRA, an author of the Monitor stated: "Patient safety is our highest priority. The Covid-19 vaccines were approved after a rigorous review of the safety, quality, and effectiveness of the vaccines by the MHRA and the CHM. The MHRA concluded that the Covid 19 vaccines were safe and effective, and the benefits of the vaccines outweigh any risks." And this mantra has continued into its 5th year even though they have YCVM evidence of harm.
CONCLUSION
Given the well-documented SAEs and unacceptable harm-to-reward ratio, governments should be urged to endorse and enforce a global moratorium on these modified mRNA products.
We should take great interest in the MHRA, which is responsible for the pharmacovigilance of the Covid–19 "vaccines", a brand-new experimental technology. We should be particularly interested in the recording of information surrounding these liability-free vaccines. As members of the public, we should have substantial interest in reviewing the monitoring of these vaccines by the MHRA, introduced via an untested, accelerated review process.
I believe there is a very strong need for the public to be made aware of this available data and it should be used to update the advice given especially to those who are pregnant.
The MHRA's answers are uninformed, and therefore, they are not telling the public the truth. This occasions a lack of trust in their ability to protect the public from harmful substances.
Lack of trust of the MHRA develops because of its duplicitous and disingenuous behaviour, demonstrated at its board meetings and appearances on other platforms.
The MHRA has demonstrated malfeasance in public office.
I conclude with a quote from the British Medical Journal, editorialised in January 2022:
"Pharmaceutical companies are reaping vast profits without adequate independent scrutiny of their scientific claims. The purpose of regulators is not to dance to the tune of rich global corporations and enrich them further; it is to protect the health of their populations. We need complete data transparency for all studies, we need it in the public interest, and we need it now".
It is something I will never come to terms with that children and pregnant women were targeted with this experimental substance. People were so blindly trusting of the corrupted institutions that have been completely compromised, they lie as easily as they breathe. Ethical and moral standards left the building a long time ago and the majority of the public are still living in ignorance and have not caught up with the criminal enterprises that are surrounding them.
Thanks you Cheryl for your fantastic perisitence in chasing FOIs. Your findings highlight the woeful inadequacies of the MHRA.